WOUND HEALING
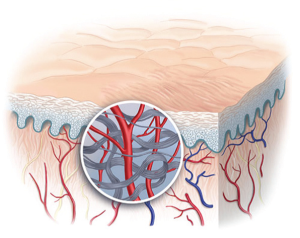 The primary function of the skin is to serve as a protective barrier against the environment. Loss of the integrity of large portions of the skin as a result of injury or illness may lead to major disability or even death.
The primary function of the skin is to serve as a protective barrier against the environment. Loss of the integrity of large portions of the skin as a result of injury or illness may lead to major disability or even death.
Skin-wound healing starts immediately after injury and consists of three phases:
1) Inflammation
2) Proliferation and
3) Maturation
These phases proceed with complicated but well-organized interaction between various tissues and cells. Various cellular and molecular-biological studies demonstrated that many cytokines, growth factors, and proteases are closely involved in the wound-healing process to complete normal tissue repair after damage.
However, the wound healing process is not linear and can progress forward and backward through the phases depending on various intrinsic and extrinsic factors.
Inflammatory phase
The inflammatory phase is characterized by its cardinal signs:
1) Rubor (Redness)
2) Calor (Warmth)
3) Tumor (Swelling)
4) Dolor (Pain) and
5) Functio laesa (Loss of function)
In normal healing process, immediately after the acute skin injury, hemostatic mechanisms and pathways commence. The initiation of the extrinsic coagulation cascade starts due to injury to vascular tissue with reflex vasoconstriction. Tissue factors and calcium activate factor VII and subsequently the whole coagulation cascade, with final blood clotting and vasoconstriction. This prevents further blood losses.
However, many mediators connected with the coagulation process (proteins of coagulation cascade, platelet-derived factors, and local hormones) also initiate processes of local inflammation. After initial vasoconstriction, the classic signs of inflammation are manifested from increased vascular permeability.
Rubor (redness) results from vasodilation, mediated by prostacyclin, prostaglandin A, prostaglandin D, and prostaglandin E (PGE).
Tumor (swelling) is due to increased vascular permeability as vascular endothelial gaps enlarge, allowing an escape of plasma proteins and fluid into the interstitial space. These changes are potentiated by PGE2 and prostaglandin F2α and support the ingress of inflammatory cells into the area of injury. This also leads to an increase in local temperature (calor), which supports an environment that is hostile to micro-organisms. Dolor (pain) is sensed as prostacyclin, PGE, and PGE2 act on peripheral nociceptors.
At this stage the process creates a barrier against microbial invasion that is potentiated by all types of white blood cells (WBC) and macrophages. Even pain plays an important role because it decreases the activity of the injured part of the body.
Inflammation also starts the healing process. Toward the end of the inflammatory cycle, the evolving milieu of eicosanoids in the wound interacts with the present cell types, resulting in fibroblast synthesis of collagen and ground substance (from the increased ratio of prostaglandin F2α to PGE2). In addition, the macrophage-derived growth factors are at optimal levels, strongly influencing the influx of first fibroblasts, keratinocytes, and then endothelial cells into the wound. As mononuclear cells continue to replace white blood cells and macrophages, the proliferative phase begins.
Role of inflammation in scar formation
Wound healing is always connected with fibrosis and subsequent scar formation. Scar tissue remains weaker than normal skin with an altered extracellular matrix composition.
Scarless wounds are characterized by a relative lack of inflammation. Furthermore, the introduction of inflammation into scarless wounds produces dose-dependent increases in wound macrophages, neutrophils, collagen deposition, and scarring. This suggests an important role of inflammation in scar formation.
Proliferative phase
The proliferative phase essentially involves the generation of the repair material. The fibroblasts are the dominant cell type in the wounded tissue. They start migrating inward from wound margins over the fibrinous matrix. They are stimulated by basic fibroblast growth factor (bFGF) and tumor growth factor-b from macrophages and platelet derived growth factor (PDGF) from platelets. In the first week, fibroblasts produce glycosaminoglycans (hyaluronic acid), proteoglycans, and collagen; these products are the main extracellular substances of granulation tissue.
Collagen is the major component of acute wound connective tissue, with net production continuing for nearly 6 weeks.
The proliferation of keratinocytes and endothelial cells produce autocrine growth factors that maintain their growth. Synchronous endothelial expansion contributes to angiogenesis as intact vessels and generates buds in granulation tissue. Neovascularization facilitates growth of the advancing line of fibroblasts into the wound, providing them with necessary nutrients and cytokines.
The degradation of the fibrin clot and provisional matrix is accompanied by the deposition of granulation tissue which continues until the wound is covered. Simultaneously, epithelial cells continue to migrate inward from the wound edge until the defect is covered. Wound contraction follows, replacing injured tissue volume with new tissue. A decrease of hyaluronic acid slows down fibroblast migration and proliferation and induces fibroblast differentiation. This initiates the maturation phase of wound healing.
Maturation phase
In the formed granulation tissue (described earlier) the collagen is remodeled into a more organized structure with increased tensile strength. Tensile strength plateaus at 80% of the original strength.
Requirement for faster healing
Wound healing remains a challenging clinical problem and correct, efficient wound management is essential.
The objective in wound management is to heal the wound in the shortest possible duration, with minimal pain, discomfort and scarring to the patient.
Requirements for fastest healing are
1. Reducing or eliminating causative factors (pressure, shear friction, moisture, circulatory impairment and/or neuropathy)
2. Providing systemic support for healing (blood, oxygen, fluid nutrition, and/or antibiotics)
3. Removal of necrotic tissue or foreign body
Inflammation is protective attempt by organism to remove the injurious stimuli and to initiate the healing process.
But, inflammation has an instrinsic ability to injure normal tissues. When inflammation is inappropriately directed against self tissues or is not adequately controlled, it becomes the cause of injury and disease. Inflammatory reactions can prevent normal healing process in postoperative and post traumatic wounds.
For faster healing most important is to control the harmful cascade of inflammation yet not interfere with its beneficial effects